 Tweet
Tweet
saw this linked off NakedCapitalism
http://nihoncassandra.blogspot.com/2...ng-part-2.html
http://nihoncassandra.blogspot.com/2...ng-part-2.html
The Price is...ummm....errrr.... Wrong (Part 2)
Many moons ago, while at university, I had a dog - a cross between a Chow-Chow and an Alsatian (the snout, eyes and dimension of the chow, with the shorter fur, muscularity, ears, and demeanor of the shepherd). Chow, as he was called, (named by a housemate at his moment of maximum apathy) had an iron constitution cultivated through years of his solo carousing, particularly his late night visits to the back of the local pizzeria, and his rummaging of the neighborhood's rubbish bins. When not on the prowl, Chow spent most of his time on our gently-sloping 4x3 meter first floor front roof - "guarding" his errr ummm....castle. He was an odd a sight - such that he became a bit of a local celebrity, and a well-loved local fixture. So, when I looked out the window and saw he'd vomited his (and our) dinner of the "freshly" caught and grilled bluefish fillets that "friends" had brought as proof of their fishing exploits, I suspected that I, too, might soon meet a similar fate.
Food poisoning is NOT fun. Food poisoning that results from bad fish can be unspeakably horrible. Leaving out the most gruesome bits, I found myself the next scorcher-of-a-July morning with a fever rallying like the price of Silver after a bubble-vision interview with Jim Rogers, or the Bunker-Hunt's declaration that they were in possession of most of the Comex warehouse receipts. I experienced a cycle of chills and sweats such that when my then GF who was worried by my moans and climbing fever, took me to a private clinic nearby (the only one open on a Sunday morning), I left the house wrapped in blanket despite the triple-digit [fahrenheit] temperature. Not exaggerating, I was unable to sit upright in the chair in the waiting room such were the shivers and vertiginous undulations. As my friend dispensed formalities with the clerk-nurse, so I laid myself on the floor of the empty waiting room. "How would you like to pay?" queried the bespectacled overweight nurse-cum-bouncer in the most deadpan of tones. "Errrr, can't we do this after?" my friend said, "I mean, look at him (pointing to me on the floor) he's, like, pretty bad". Receptionist replied (expressionless again) as if she was uttering the most normal thing in the world: "No, you cannot see the doctor until you have paid." "I'll write her a check", I managed between groans, having followed the conversation between the near- hallucinations (the kind that makes one maniacal about Ayn Rand as described in Tobias Wolff's"Old School"), the chills and the somersaulting of the waiting room. Nurse-Bouncer return-volleyed: "I am sorry, we don't take personal checks". "WTF....WTFFingF.....@%$!! Was all I could utter, though it is unclear how comprehensible it was, if audible at all. Suffice to say, this was Sunday, mid-day, in the low-rent 'burbs, before cell-phones, before the internet, before ubiquitous ATMs, before debit cards, and at a time when credit cards were hardly inventory in the typical undergraduate student's billfold. So I lay there, shivering as if I were atop the Eiger in January, despite the 100F heat and mid-summer humidity outside. Fortunately, payment was sorted out by a phone-call to GFs mother who was kind enough to send eldest sister down with funds. Welcome to the American Healthcare System!, I cursed afterwards. In hindsight, I should have gone to the hospital, but at THAT time, our belief was that The Hospital (with upper-case "H") was reserved for CRITICAL things - a limb being sewn back on it's owner, brain surgery, C-section births, removing buckshot from Dick Cheney's ass, gunshot and/or stab wounds and the like. I still shake my head and ask whether it really happened, but it did - just as described.
Time-leap nearly three decades forward. Eldest daughter recently had a heart scare during athletics, in the UK. Nothing critical, but something unknown which begged investigation. The attending GP suggested that she see a specialist. By nature of her residence, she's covered by the NHS. Rationing queue meant the earliest appointment was six weeks. However, if she wanted to jump the queue, the specialist will see her privately immediately. Cost? GBP800. That is just for the consultation - presumably (though not assuredly) including the ECG & stress test(s). Rather than be pick-pocketed by over-enterprising UK cardiologist, we are able to get an appointment at a private practice near our home in France (BTW, contrary to popular belief in the US and the UK, all practices in France are private) in two weeks coinciding with her next visit home. She undergoes a thorough exam, stress tests and ECG. Useful but inconclusive. Cost? GBP100. (Note: That is not the co-payment. That is the invoiced amount!!). In the absence of seeing her when another episode might arises, he recommends an MRI (with hi-tech contrast media etc.) to rule out the worst. We make an appointment (also at a private clinic) for two-days hence. Tests are completed. New machines. Super high-tech gear. Cost? GBP125, inclusive of radiographer's reading and opinion. This is, again, NOT the co-pay (in US lingo), but the private price to the customer. This is the usual and customary cost reimbursed by the State Single Payer. They extend the same price to me without question, so I don't have to be Kaiser Permanente to obtain their volume discount. Each visit type or procedure has a price. That is that. Full transparency. Not one price for the insurance company and the other "retail walk-in's". One price. One of my children had a small tongue-tie clipped at a suburban New York hospital. The anaesthesiologist alone charged $800 (and that was 10 years ago) for the 10-minutes and two-jokes (not including the cost of the anaesthetic itself), while the full procedure was $6000 (retail, walk-in, rack-rate price). In France they do this as an outpatient procedure in the ENT surgeon's office with a local anaesthetic, for less than a twentieth of the price. I can only imagine what my daughter's same two cardiological and radiological consultations and procedures would have cost in the US (but would be fascinated whether anyone knows the range of prices one might encounter).
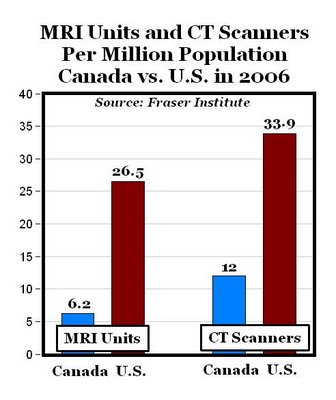
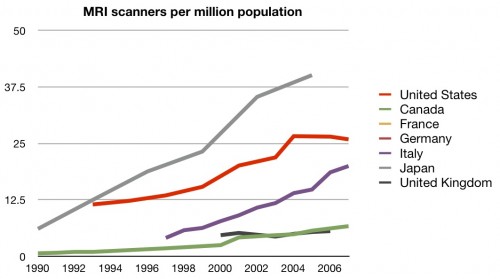
The troubling thing to an Economist (or me at least, lest I shame Economists if such a thing were possible), is the sheer discrepancy between these actual prices. These are factors of 6x between the private UK price and private French price (even before the USA weighs in). We are not talking about a hospital in India where the reward for saving 75% on your procedure is an untreatable staphylococcus infection that might very-well kill you. Remember, the French cardiologists and radiologists are private. They are running businesses. They are free to charge what they want. Their equipment is not subsidized, so presumably the fees per scan and payback periods of their MRI scanner must make some economic sense. This is not Greece or Portugal sovereign, and French banks are notoriously hard-nosed with domestic small business customers who get their sums wrong (unlike the lax scrutiny they gave to Europe's peripheral sovereigns. Admittedly, prices in the 16th of Paris would be somewhat higher, but nonetheless my region is one of the wealthiest in France. So one might ask, Why is this so?
Well for a start, French doctors and specialists are probably underpaid. But they are not starving, though they are clearly bearing some of the difference, particularly GPs and Dentists. Why don't they just charge more? Well, for one, most people wouldn't pay or couldn't pay, and would seek out the provider charging the usual and customary reimbursed by the Single Payor. France also has a single nationwide healthcare IT system interfacing with all providers which is a huge advantage, both from a cost and ability to track fraud point of view. And the The Single Payor has the entire risk pool, which prevents the state from getting all the expensive chronic conditions, and the private sector cherry-picking the good risk, and privatizing (i.e. pocketing most or the majority of the fatter underwriting profit), and so not passing it on the insured person, or the state who is the ultimate underwriter. And of course the State does get the chronic conditions. And happily so, because its all well and good for Libertarians to say this is "unfair" to the healthy or the young, who are paying more than they actuarily should (in isolation), except one never knows when or who chronic will strike, and it could be YOU. Americans have never grasped this democratic fact, sufficiently to make generational sharing a priority. The concept of a "pre-existing condition" doesn't exist in France. The insured cost IS socialized, by design (and efficiently so!) and for the overwhelming majority (excepting those with private planes), everyone is better off. There is NO ONE in the French Healthcare civil service earning anywhere close to what directors and senior officers at private US HMOs, Health Insurers, and Hospital Groups extract from patients, corporate customers, taxpayers and shareholders. By an unimaginably huge factor. No one (least of all the CEOs, Directors, and managers of the French Healthcare infrastructure) has suggested that the French State "Demutualize", as they did in the US (driven by the lure of exceptional parochial gain. Even the Private providers of French "Top-Up" Health Insurance are dominated by private but non-profit mutuals. The largesse of corporate health insurance hierarchies are not reproduced over-and-over so that there are fewer pigs at the trough extracting for their private benefit, every healthcare dollar they can seize, which is the apparent SOP in the USA. The French run a utilitarian ship, without having their board meetings in exotic places, or the award of share options for doing what they are paid to do: their job. And it shows. Perhaps it's too utilitarian, but it is clear (unless you are in the business of surgically extracting dollars from the various constituents) which side the public-as-financier and benefactor should err on.
Does this make the French stupid for not more aggressively taking advantage of extraction opportunities? What by implication does this say about the USA? France spends approximately 12% of GDP for which citizens receive universal coverage, better outcomes, full choice of providers, total portability, no rationing, and most important perhaps, no exclusions. This is more spending than the UK NHS's 9% but 7% of GDP LESS than the USA's fragmented, byzantine system, so weird and absurd that you couldn't design it as such, or replicate it if you tried. That is 7% of $14 trillion GDP or the equivalent of spending approximately a trillion dollars (yes $1,000,000,000,000) LESS and achieving SUBSTANTIALLY MORE. Because this is a rather important point, it bears repeating again (and again!). Universal coverage (i.e., yes, Everyone); Complete Freedom of Choice (you can visit any doctor you choose); Prescription Meds covered with nominal co-pays. NO EXCLUSIONS FOR PRE-EXISTING CONDITIONS (one never knows who may afflicted next, defeating the entire purpose of "insurance"). Complete portability (i.e.. no worries when you change jobs or if get fired). Reimbursement for alternative therapies (Naturopathy, acupuncture, prevention, etc.), latest technology in more or less similar proportions as the US, and separate extended-coverage insurance offered by the private market to pay for private rooms, vision care, top specialists, fashion eyewear, travel health insurance, etc. - all for 7% of GDP LESS spend than the USA. Medicare-like "insurance", that primarily pays the bills of Gran's third hip replacement, Pap's coronary roto-rootering or by-pass, or daily Lipitor ration, but doesn't level the cost across the risk-pool over one's life-cycle can hardly be called insurance, but rather are just direct transfer payments under the guise of "insurance". France, by contrast, levies social security taxes upon all (attenuated by ability to pay), set at something which equates to one's share of the expenditure across the whole population. There are shortfalls to be certain, but these are measured in numbers with zeros that remain tethered to reality and bridgeable. Everyone who can must contribute by law according to a strict schedule, for which in return, citizens are legally entitled to coverage. It is a crackingly good, fair, not to mention pragmatic approach to the problem.
Yet, champions of the US system will still claim its "better", and are afraid of losing what they have. When my father was diagnosed with lung-cancer, his Health insurance company refused to pay for the Tarceva prescribed by his attending cancer specialist. Tarceva is VERY expensive. And admittedly, it is for most, rarely a cure. Yet the specialist, (at the Ivy teaching hospital) who was one of the top specialists in the field of the type of cancer he was treating, prescribed the medicine and was told by the insurance company that they will not pay. The prescription was based upon the patient's cancer's likely sensitivity to the compound. THAT is the much-vaunted US Healthcare system: rife with conflicts of interest; maximum extraction, no transparency, little logic that is not parochially self-serving. When I went to my local pharmacy (here in France) and explained my father's situation to my friendly pharmacist, she just couldn't understand, and looked at me as if I was from Mars. It was inconceivable to her. In her world, if the doctor is licensed, he is presumed to know best. The Single-payor is obliged to pay for the procedures and medicines the doctor prescribes. No questions (unless there is fraud or ethical situation). Apologists for US Healthcare Byzantium will point out the possibility of fraud and abuse. Let it be said: there is abuse and fraud. But is remains the exception rather than the rule, and even with abuse and fraud included they still spend only 12% of GDP on Healthcare. Yes ~12% vs. US ~19%.
But perhaps, the French are just be Healthier?. The outcome statistics could be masking what are essentially lifestyle and societal differences: better diet, more exercise, less processed food, universal coverage that encourages preventive care and early detection that, in a virtuous circle, lower costs. But the French smoke like chimneys and drink alcohol like camels at an oasis after a Sahara crossing. They eat food that often is more fat than anything else (for breakfast, lunch, and dinner). And obesity is rising rapidly here too. But they do eat better (more fresh veg, and lots of fresh fruit). They eat seasonally. Their coffees are measured by the thimble, they they have more of them, while the concept of the Big Gulp, and Supersize meals, meet with amusement and derision, despite the growing popularity of Starbucks and ubiquity of McDonalds. To be sure the reasons are numerous, and while a factor, lifestyle while important, is probably not dominant.
It is surprising that France has not become a destination for healthcare tourists. It is surprising that in the UK, there is no middle ground between public and private healthcare such that one's NHS benefit is not applied to one's private visit. But it is more surprising (and alarming) that socialized medicine (a misnomer if ever there was one when applied to France) is met with derision by most, and that America doesn't look to emulate the better organized healthcare systems in developed nations around the globe. Sure there are dedicated professionals who should be lauded. But they exist elsewhere too. I look in earnest for the virtues of the American healthcare system, and they are systemically absent, save my old highly-competent NYC dentist who charged a very reasonable rate for my visits - so long as it was in cash. A Saint? An altruist? Nope, just four ex-wives with a claim on every reported depreciating dollar....
Many moons ago, while at university, I had a dog - a cross between a Chow-Chow and an Alsatian (the snout, eyes and dimension of the chow, with the shorter fur, muscularity, ears, and demeanor of the shepherd). Chow, as he was called, (named by a housemate at his moment of maximum apathy) had an iron constitution cultivated through years of his solo carousing, particularly his late night visits to the back of the local pizzeria, and his rummaging of the neighborhood's rubbish bins. When not on the prowl, Chow spent most of his time on our gently-sloping 4x3 meter first floor front roof - "guarding" his errr ummm....castle. He was an odd a sight - such that he became a bit of a local celebrity, and a well-loved local fixture. So, when I looked out the window and saw he'd vomited his (and our) dinner of the "freshly" caught and grilled bluefish fillets that "friends" had brought as proof of their fishing exploits, I suspected that I, too, might soon meet a similar fate.
Food poisoning is NOT fun. Food poisoning that results from bad fish can be unspeakably horrible. Leaving out the most gruesome bits, I found myself the next scorcher-of-a-July morning with a fever rallying like the price of Silver after a bubble-vision interview with Jim Rogers, or the Bunker-Hunt's declaration that they were in possession of most of the Comex warehouse receipts. I experienced a cycle of chills and sweats such that when my then GF who was worried by my moans and climbing fever, took me to a private clinic nearby (the only one open on a Sunday morning), I left the house wrapped in blanket despite the triple-digit [fahrenheit] temperature. Not exaggerating, I was unable to sit upright in the chair in the waiting room such were the shivers and vertiginous undulations. As my friend dispensed formalities with the clerk-nurse, so I laid myself on the floor of the empty waiting room. "How would you like to pay?" queried the bespectacled overweight nurse-cum-bouncer in the most deadpan of tones. "Errrr, can't we do this after?" my friend said, "I mean, look at him (pointing to me on the floor) he's, like, pretty bad". Receptionist replied (expressionless again) as if she was uttering the most normal thing in the world: "No, you cannot see the doctor until you have paid." "I'll write her a check", I managed between groans, having followed the conversation between the near- hallucinations (the kind that makes one maniacal about Ayn Rand as described in Tobias Wolff's"Old School"), the chills and the somersaulting of the waiting room. Nurse-Bouncer return-volleyed: "I am sorry, we don't take personal checks". "WTF....WTFFingF.....@%$!! Was all I could utter, though it is unclear how comprehensible it was, if audible at all. Suffice to say, this was Sunday, mid-day, in the low-rent 'burbs, before cell-phones, before the internet, before ubiquitous ATMs, before debit cards, and at a time when credit cards were hardly inventory in the typical undergraduate student's billfold. So I lay there, shivering as if I were atop the Eiger in January, despite the 100F heat and mid-summer humidity outside. Fortunately, payment was sorted out by a phone-call to GFs mother who was kind enough to send eldest sister down with funds. Welcome to the American Healthcare System!, I cursed afterwards. In hindsight, I should have gone to the hospital, but at THAT time, our belief was that The Hospital (with upper-case "H") was reserved for CRITICAL things - a limb being sewn back on it's owner, brain surgery, C-section births, removing buckshot from Dick Cheney's ass, gunshot and/or stab wounds and the like. I still shake my head and ask whether it really happened, but it did - just as described.
Time-leap nearly three decades forward. Eldest daughter recently had a heart scare during athletics, in the UK. Nothing critical, but something unknown which begged investigation. The attending GP suggested that she see a specialist. By nature of her residence, she's covered by the NHS. Rationing queue meant the earliest appointment was six weeks. However, if she wanted to jump the queue, the specialist will see her privately immediately. Cost? GBP800. That is just for the consultation - presumably (though not assuredly) including the ECG & stress test(s). Rather than be pick-pocketed by over-enterprising UK cardiologist, we are able to get an appointment at a private practice near our home in France (BTW, contrary to popular belief in the US and the UK, all practices in France are private) in two weeks coinciding with her next visit home. She undergoes a thorough exam, stress tests and ECG. Useful but inconclusive. Cost? GBP100. (Note: That is not the co-payment. That is the invoiced amount!!). In the absence of seeing her when another episode might arises, he recommends an MRI (with hi-tech contrast media etc.) to rule out the worst. We make an appointment (also at a private clinic) for two-days hence. Tests are completed. New machines. Super high-tech gear. Cost? GBP125, inclusive of radiographer's reading and opinion. This is, again, NOT the co-pay (in US lingo), but the private price to the customer. This is the usual and customary cost reimbursed by the State Single Payer. They extend the same price to me without question, so I don't have to be Kaiser Permanente to obtain their volume discount. Each visit type or procedure has a price. That is that. Full transparency. Not one price for the insurance company and the other "retail walk-in's". One price. One of my children had a small tongue-tie clipped at a suburban New York hospital. The anaesthesiologist alone charged $800 (and that was 10 years ago) for the 10-minutes and two-jokes (not including the cost of the anaesthetic itself), while the full procedure was $6000 (retail, walk-in, rack-rate price). In France they do this as an outpatient procedure in the ENT surgeon's office with a local anaesthetic, for less than a twentieth of the price. I can only imagine what my daughter's same two cardiological and radiological consultations and procedures would have cost in the US (but would be fascinated whether anyone knows the range of prices one might encounter).
The troubling thing to an Economist (or me at least, lest I shame Economists if such a thing were possible), is the sheer discrepancy between these actual prices. These are factors of 6x between the private UK price and private French price (even before the USA weighs in). We are not talking about a hospital in India where the reward for saving 75% on your procedure is an untreatable staphylococcus infection that might very-well kill you. Remember, the French cardiologists and radiologists are private. They are running businesses. They are free to charge what they want. Their equipment is not subsidized, so presumably the fees per scan and payback periods of their MRI scanner must make some economic sense. This is not Greece or Portugal sovereign, and French banks are notoriously hard-nosed with domestic small business customers who get their sums wrong (unlike the lax scrutiny they gave to Europe's peripheral sovereigns. Admittedly, prices in the 16th of Paris would be somewhat higher, but nonetheless my region is one of the wealthiest in France. So one might ask, Why is this so?
Well for a start, French doctors and specialists are probably underpaid. But they are not starving, though they are clearly bearing some of the difference, particularly GPs and Dentists. Why don't they just charge more? Well, for one, most people wouldn't pay or couldn't pay, and would seek out the provider charging the usual and customary reimbursed by the Single Payor. France also has a single nationwide healthcare IT system interfacing with all providers which is a huge advantage, both from a cost and ability to track fraud point of view. And the The Single Payor has the entire risk pool, which prevents the state from getting all the expensive chronic conditions, and the private sector cherry-picking the good risk, and privatizing (i.e. pocketing most or the majority of the fatter underwriting profit), and so not passing it on the insured person, or the state who is the ultimate underwriter. And of course the State does get the chronic conditions. And happily so, because its all well and good for Libertarians to say this is "unfair" to the healthy or the young, who are paying more than they actuarily should (in isolation), except one never knows when or who chronic will strike, and it could be YOU. Americans have never grasped this democratic fact, sufficiently to make generational sharing a priority. The concept of a "pre-existing condition" doesn't exist in France. The insured cost IS socialized, by design (and efficiently so!) and for the overwhelming majority (excepting those with private planes), everyone is better off. There is NO ONE in the French Healthcare civil service earning anywhere close to what directors and senior officers at private US HMOs, Health Insurers, and Hospital Groups extract from patients, corporate customers, taxpayers and shareholders. By an unimaginably huge factor. No one (least of all the CEOs, Directors, and managers of the French Healthcare infrastructure) has suggested that the French State "Demutualize", as they did in the US (driven by the lure of exceptional parochial gain. Even the Private providers of French "Top-Up" Health Insurance are dominated by private but non-profit mutuals. The largesse of corporate health insurance hierarchies are not reproduced over-and-over so that there are fewer pigs at the trough extracting for their private benefit, every healthcare dollar they can seize, which is the apparent SOP in the USA. The French run a utilitarian ship, without having their board meetings in exotic places, or the award of share options for doing what they are paid to do: their job. And it shows. Perhaps it's too utilitarian, but it is clear (unless you are in the business of surgically extracting dollars from the various constituents) which side the public-as-financier and benefactor should err on.
Does this make the French stupid for not more aggressively taking advantage of extraction opportunities? What by implication does this say about the USA? France spends approximately 12% of GDP for which citizens receive universal coverage, better outcomes, full choice of providers, total portability, no rationing, and most important perhaps, no exclusions. This is more spending than the UK NHS's 9% but 7% of GDP LESS than the USA's fragmented, byzantine system, so weird and absurd that you couldn't design it as such, or replicate it if you tried. That is 7% of $14 trillion GDP or the equivalent of spending approximately a trillion dollars (yes $1,000,000,000,000) LESS and achieving SUBSTANTIALLY MORE. Because this is a rather important point, it bears repeating again (and again!). Universal coverage (i.e., yes, Everyone); Complete Freedom of Choice (you can visit any doctor you choose); Prescription Meds covered with nominal co-pays. NO EXCLUSIONS FOR PRE-EXISTING CONDITIONS (one never knows who may afflicted next, defeating the entire purpose of "insurance"). Complete portability (i.e.. no worries when you change jobs or if get fired). Reimbursement for alternative therapies (Naturopathy, acupuncture, prevention, etc.), latest technology in more or less similar proportions as the US, and separate extended-coverage insurance offered by the private market to pay for private rooms, vision care, top specialists, fashion eyewear, travel health insurance, etc. - all for 7% of GDP LESS spend than the USA. Medicare-like "insurance", that primarily pays the bills of Gran's third hip replacement, Pap's coronary roto-rootering or by-pass, or daily Lipitor ration, but doesn't level the cost across the risk-pool over one's life-cycle can hardly be called insurance, but rather are just direct transfer payments under the guise of "insurance". France, by contrast, levies social security taxes upon all (attenuated by ability to pay), set at something which equates to one's share of the expenditure across the whole population. There are shortfalls to be certain, but these are measured in numbers with zeros that remain tethered to reality and bridgeable. Everyone who can must contribute by law according to a strict schedule, for which in return, citizens are legally entitled to coverage. It is a crackingly good, fair, not to mention pragmatic approach to the problem.
Yet, champions of the US system will still claim its "better", and are afraid of losing what they have. When my father was diagnosed with lung-cancer, his Health insurance company refused to pay for the Tarceva prescribed by his attending cancer specialist. Tarceva is VERY expensive. And admittedly, it is for most, rarely a cure. Yet the specialist, (at the Ivy teaching hospital) who was one of the top specialists in the field of the type of cancer he was treating, prescribed the medicine and was told by the insurance company that they will not pay. The prescription was based upon the patient's cancer's likely sensitivity to the compound. THAT is the much-vaunted US Healthcare system: rife with conflicts of interest; maximum extraction, no transparency, little logic that is not parochially self-serving. When I went to my local pharmacy (here in France) and explained my father's situation to my friendly pharmacist, she just couldn't understand, and looked at me as if I was from Mars. It was inconceivable to her. In her world, if the doctor is licensed, he is presumed to know best. The Single-payor is obliged to pay for the procedures and medicines the doctor prescribes. No questions (unless there is fraud or ethical situation). Apologists for US Healthcare Byzantium will point out the possibility of fraud and abuse. Let it be said: there is abuse and fraud. But is remains the exception rather than the rule, and even with abuse and fraud included they still spend only 12% of GDP on Healthcare. Yes ~12% vs. US ~19%.
But perhaps, the French are just be Healthier?. The outcome statistics could be masking what are essentially lifestyle and societal differences: better diet, more exercise, less processed food, universal coverage that encourages preventive care and early detection that, in a virtuous circle, lower costs. But the French smoke like chimneys and drink alcohol like camels at an oasis after a Sahara crossing. They eat food that often is more fat than anything else (for breakfast, lunch, and dinner). And obesity is rising rapidly here too. But they do eat better (more fresh veg, and lots of fresh fruit). They eat seasonally. Their coffees are measured by the thimble, they they have more of them, while the concept of the Big Gulp, and Supersize meals, meet with amusement and derision, despite the growing popularity of Starbucks and ubiquity of McDonalds. To be sure the reasons are numerous, and while a factor, lifestyle while important, is probably not dominant.
It is surprising that France has not become a destination for healthcare tourists. It is surprising that in the UK, there is no middle ground between public and private healthcare such that one's NHS benefit is not applied to one's private visit. But it is more surprising (and alarming) that socialized medicine (a misnomer if ever there was one when applied to France) is met with derision by most, and that America doesn't look to emulate the better organized healthcare systems in developed nations around the globe. Sure there are dedicated professionals who should be lauded. But they exist elsewhere too. I look in earnest for the virtues of the American healthcare system, and they are systemically absent, save my old highly-competent NYC dentist who charged a very reasonable rate for my visits - so long as it was in cash. A Saint? An altruist? Nope, just four ex-wives with a claim on every reported depreciating dollar....






Comment